Tibiofibular Joint Instability
What is the proximal tibiofibular joint?
The proximal tibiofibular joint is located between the lateral tibial plateau of the tibia (shinbone), and the head of the fibula (small long bone on the outside of the leg).
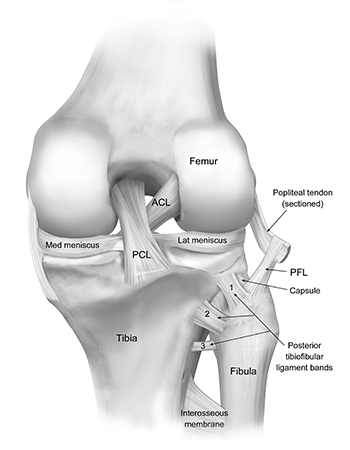
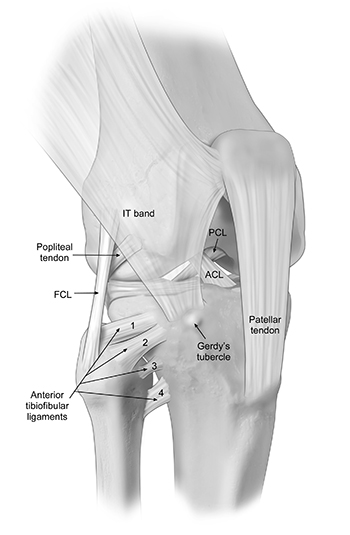
Classically, the proximal tibiofibular joint is injured in a fall when the foot is downwards (ankle is plantar-flexed), with the stress being brought through the fibula, will cause the proximal fibula to sublux (partial dislocation) out of place over the lateral aspect of the knee joint. In other circumstances, significant trauma or a motor vehicle accident can cause a disruption of the proximal tibiofibular joint. In most circumstances, it is the posterior proximal tibiofibular joint ligament that is injured. This results in the fibula rotating away from the tibia during deep squatting.
The symptoms of a proximal tibiofibular instability can vary depending on the severity of the injury, but common signs and symptoms include:
- Pain: Pain around the knee is a primary symptom. The intensity of the pain may vary, but it is typically aggravated by movement or putting weight on the affected leg or when rotating the leg.
- Instability: This can be perceived as motion or true dislocation of the fibular head on the tibia.
- Deformity: In more severe cases the fibular head can be dislocated an observed through the skin.
- Crepitus: Some individuals may experience a grating or crunching sensation (crepitus) when osteoarthritis has developed.
The combination of a detailed history, comprehensive physical examination, x-rays, and possibly an MRI is the key to a successful diagnosis of a proximal tibiofibular instability. Dr. Jorge Chahla and his team will complete a thorough exam to evaluate your range of motion, stability, and points of tenderness to palpation. Specifically, in acute cases, it is sometimes challenging to make the patient relax sufficiently to be able to examine for proximal tibiofibular joint instability, but usually having the knee flexed to 90 degrees and trying to perform an anterolateral subluxation maneuver of the proximal tibiofibular joint is sufficient to confirm this diagnosis. In chronic injuries, the instability may appear obvious when the patient performs a maximal squat. It is always important to perform the exam on both legs to ensure that there is a significant difference from one side to the other. In more chronic cases, we have the patient squat down, which can often demonstrate that the proximal tibiofibular joint is being subluxed. Concurrent with this, we will perform a Tinel’s test by percussing over the common peroneal nerve to confirm the presence of dysesthesias or “zingers,” which translate down the leg. X-rays will be obtained to allow Dr. Chahla to assess the position of the fibular head. An MRI may be ordered to observe the anterior and posterior ligamentous complexes.
The tibiofibular joint plays a crucial role in stabilizing the knee and lower leg, allowing for proper movement and weight distribution. Tibiofibular joint instability can result from trauma, ligament injuries, or chronic overuse, leading to pain, swelling, and instability in the knee or lower leg. If left untreated, this condition can impact mobility and athletic performance. Dr. Jorge Chahla, a leading orthopedic knee surgeon, specializes in diagnosing and treating tibiofibular joint instability, helping patients regain stability and function. If you are experiencing persistent knee or lower leg pain, schedule an appointment with Dr. Chahla in Chicago, Naperville, or Oak Brook for expert evaluation and treatment.
At a Glance
Dr. Jorge Chahla
- Triple fellowship-trained sports medicine surgeon
- Performs over 800 surgeries per year
- Associate professor of orthopedic surgery at Rush University
- Learn more