MCL Injuries
What is the medial collateral ligament (MCL)?
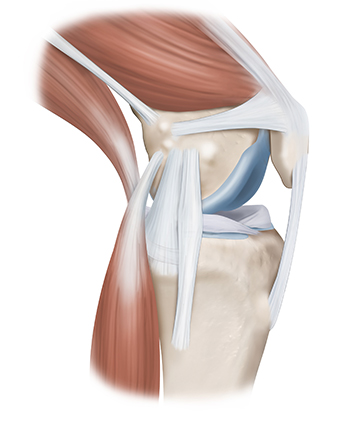
The MCL is a structure that stabilizes the medial side (inside) of the knee, connecting the thigh bone (femur) to the shinbone (tibia). The MCL prevents forces applied to the lateral (outside) side of the knee from gapping open the inside of the knee (valgus stress).
The posteromedial corner of the knee is comprised of the MCL and the posterior oblique ligament (POL). Both structures control the stability and valgus stress of the knee.
The MCL and the POL prevent the knee from gapping open when the tibia internally rotates. The MCL functions when the knee is slightly flexed (20 to 30 degrees of flexion) whereas the POL (more to the back of the knee) functions close to extension (0 degrees of flexion). The different roles of each of these ligaments help to ensure the stability of the knee to valgus stress throughout a full range of motion.
MCL injuries can result from twisting injuries, causing the knee to buckle and gap open on the inside of the knee. MCL injuries can also result from contact injuries, like a blow to the outside of the knee, causing valgus gapping. MCL injuries are very common with almost 750,000 injuries occurring every year in the United States. Overall, MCL tears are two to three times more common than ACL tears.
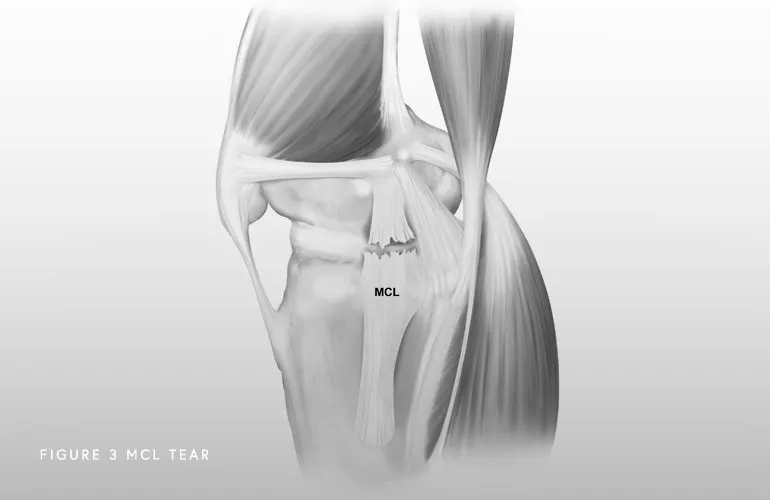
Symptoms depend on the severity of the injury. A mild injury (grade I or II) might present with pain over the ligament attachments. In more severe cases, patients feel that their knee can give out or buckle. Below are some of the most common symptoms of an MCL injury:
- Pain: Pain on the inner side of the knee is a common symptom of a torn MCL. The pain may range from mild to severe, depending on the extent of the injury.
- Swelling
- Stiffness: The knee may become stiff, making it difficult to fully bend or straighten the leg.
- Instability: An individual with a torn MCL may feel that the knee is unstable, as if it’s “giving way” or unable to support their weight properly.
- Bruising: Bruising can develop around the site of the MCL tear, and the discoloration is often seen on the inner side of the knee.
- Difficulty Walking: Walking may be uncomfortable or painful, particularly if the MCL tear is severe.
- Popping or Clicking Sensation: Some people report a popping or clicking sensation when the injury occurs, which may be followed by pain and swelling.
A combination of a comprehensive physical examination, special x-rays, and an MRI are usually very accurate. Dr. Jorge Chahla and his team will perform a physical exam that will include testing your knee in an extended (straight) and flexed position to determine the location and severity of the injury. A special x-ray, called a valgus stress x-ray, will likely be obtained. This special x-ray allows Dr. Chahla to objectively quantify and diagnose (based on validated systems) a posteromedial corner injury with millimeter accuracy. An MRI will allow Dr. Chahla to further evaluate the extent of the MCL injury as well as to evaluate the knee for any concomitant ligament, meniscal, or cartilage injuries.

The medial collateral ligament (MCL) is one of the key stabilizers of the knee, located on the inner side of the joint. MCL injuries commonly result from direct impact or excessive twisting, leading to pain, swelling, and knee instability. Dr. Jorge Chahla, a highly experienced orthopedic knee surgeon, offers specialized care for MCL injuries, ensuring patients receive the most effective treatment for their condition. If you have suffered an MCL injury, contact Dr. Chahla’s office in Chicago, Naperville, or Oak Brook to begin your recovery.
At a Glance
Dr. Jorge Chahla
- Triple fellowship-trained sports medicine surgeon
- Performs over 800 surgeries per year
- Associate professor of orthopedic surgery at Rush University
- Learn more