Imaging of the knee joint
The knee is one of the most commonly injured joints in the human body, especially in the setting of sports injuries. Sudden twisting movements that place torsional stress on the joint with the foot in a fixed position often result in meniscal or ligament damage. Some of the most common injuries to the knee involve the anterior cruciate ligament (ACL) and the medial meniscus. Imaging is an essential step in the diagnostic process, allowing non-invasive visualization of internal structures. Radiographs (x-rays) are often the first-line imaging in acute trauma settings. These demonstrate the bones but do not reveal many critical soft tissue abnormalities such as ACL or meniscus tears which often require surgical intervention. MRI (Magnetic Resonance Imaging) has become the standard for non-invasive medical imaging of the most important soft tissue structures of the knee.
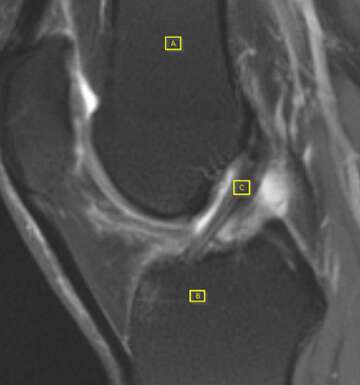
The ACL is a small 5mm thick shaped ligament (Fig. 1C) of the knee which extends between the femur (Fig. 1A) and the tibia (Fig. 1B) and functions to maintain normal bone alignment and stability at the knee. Tears of the ACL typically occur in the middle portion of the ligament, resulting in discontinuity or abnormal contour (Fig. 2C). On the T2 weighted images below, the normal ACL to the left appears as a dark (hypointense) linear band, but the torn ACL on the right appears hyperintense (brighter) and irregular.

ACL injuries vary in severity and management. Mild sprains (Grade I) result in stretching of the ACL without affecting the stability of the knee joint. Partial tears (Grade II) are uncommon and result in stretching and loosening of the ACL. Complete tears (Grade III) are the most extreme and result in complete loss of stability of the knee joint. Most grade I injuries are treated non-surgically with immobilization or bracing, physical therapy, and a gradual progression back to normal activities. Grade II/III injuries require grafting from the patellar or hamstrings tendon to ensure proper stability of the knee joint in addition to medical management.
Injuries to the ACL can be complicated by involvement of injuries of adjacent bone or soft tissue structures, such as the tibial spine. In this type of injury, the ACL itself remains intact, however the bony attachment of the ligament upon the tibia is fractured. These types of injuries usually occur in younger patients who are skeletally immature. In this T2-weighted sagittal plane image of the knee, there is tibial spine fracture and slight displacement at the ACL insertion (Fig. 3C). Above, the femur has a normal contour and intensity (Fig. 3A). Below, there is a fracture of tibial bone marrow and cortex with focal areas of hyperintensity indicating damage to the bone (Fig 3B). An avulsed bone fragment can be visualized at the base of the ACL revealing injury to the tibial eminence. Injuries to the tibial spine are graded I-IV depending on the extent of injury and degree of required intervention. While type I injuries are usually mild and can be managed conservatively, arthroscopy is recommended for the evaluation of type II-IV injuries as they may require orthopedic intervention.

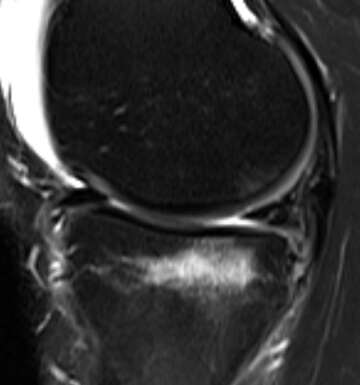
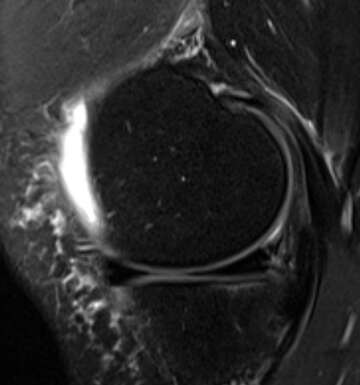
The medial meniscus is another commonly injured component of the knee. The meniscus is a crescent shaped fibrocartilaginous structure that sits in the joint space between the condyles of the femur and the tibia. The menisci function to disperse the weight of the body and reduce friction during movement, protecting the knee joint from articular cartilage damage. Early in life, the meniscus has a rich blood supply, but as aging occurs, the meniscus becomes avascular and more prone to injury. Injuries to the menisci occur when a rotational force is applied to a flexed knee, usually a twisting injury with the foot anchored to the ground. Menisci injuries are best visualized by MRI. Fig. 4 displays a normal knee joint & meniscus. The joint space between the tibia and femur is hypointense (dark) and the outer rim of the bones is clearly outlined. In Fig. 5, a hyperintense line (arrow) can be appreciated in the joint space indicating meniscal injury. Similar to the ACL, menisci injuries are graded on a 3-tier scale. Due to their avascular nature, high grade menisci injuries almost always require surgical intervention.
Biographies
Dr. Greg White is a diagnostic radiologist with subspecialty fellowship training in musculoskeletal imaging, experience and expertise in MRI imaging, and over a decade of practice experience. Research interests include imaging of sports injuries, cancer, and new applications of artificial intelligence in medical imaging.
Dr. Minhal Abidi was born in Karachi, Pakistan. At the age of five, his family immigrated to the U.S. and settled in Nashville, TN. Before graduating from the University of Tennessee with a degree in Biochemistry, Dr. Abidi served as a board member of the Oasis Center of Nashville, a local non-profit focused on promoting educational rights and social justice. His commitment to community service was maintained as a medical student at East Tennessee State University James H. Quillen College of Medicine as a volunteer at free clinics throughout rural Appalachia and by serving as a mentor to younger students. Today, he is completing his internship at Weiss Memorial Hospital in Chicago, Il, and is looking forward to joining Rush University Medical Center as a radiology resident.